Managing that load through spreadsheets, phone-based dispatch, or disconnected systems isn't a minor inconvenience — it's a structural problem. Dispatch delays, coverage gaps, and documentation errors don't stay contained. They compound.
This article covers the practical, measurable advantages EMS organizations gain when they move from manual or fragmented scheduling to purpose-built patient transport scheduling software — what changes, why it matters, and where the returns are largest.
Key Takeaways
- Patient transport scheduling software automates vehicle, crew, and route assignment based on urgency, availability, and proximity — cutting the manual phone and spreadsheet workflows dispatchers still rely on
- Faster dispatch directly affects patient outcomes: each additional minute from emergency call to first defibrillation is associated with 6% lower survival to hospital discharge
- Optimized resource assignment reduces ALS over-dispatch, idle time, and crew overtime
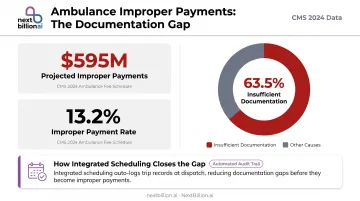
- Auto-logged trip events reduce billing exposure: CMS found 63.5% of ambulance improper payments trace back to insufficient documentation
- Mixed fleets handling both emergency and non-emergency calls see the largest efficiency gains, since automated scheduling resolves the triage and resource conflicts that manual dispatch can't keep up with
What Is Patient Transport Scheduling Software for EMS?
Patient transport scheduling software is a digital system that automates the assignment of vehicles, crews, and routes to transport requests. It matches units to patients based on urgency level, patient mobility needs, crew certifications, and real-time resource availability — replacing the manual coordination that happens over phone, radio, or whiteboard.
It's used across:
- Emergency ambulance dispatch
- Non-emergency medical transport (NEMT)
- Interfacility transfers
- Hospital discharge coordination
Worth clarifying upfront: this is an active operations layer, not a record-keeping tool. It determines how fast patients are reached, how efficiently crews are deployed, and whether an organization can scale without adding headcount just to manage coordination.
Key Advantages of Patient Transport Scheduling Software
The advantages below are grounded in operational outcomes — response performance, cost efficiency, and regulatory adherence. Each one compounds with fleet size and call volume.
Advantage 1: Faster, More Accurate Dispatch and Reduced Response Times
Manual dispatch asks a human to simultaneously track vehicle locations, crew availability, certification status, and patient acuity — then make an assignment decision. Scheduling software does that in seconds by maintaining real-time visibility across all those variables simultaneously.
The result: the time between call receipt and unit assignment drops. The nearest appropriately equipped unit that matches the patient's acuity gets dispatched automatically, without a dispatcher working through a mental checklist.
Why the time savings matter clinically:
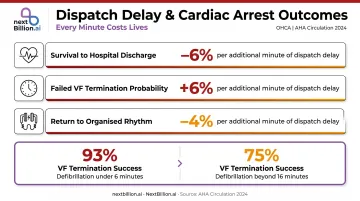
A 2024 AHA Circulation study of 3,723 witnessed out-of-hospital cardiac arrest patients found that each additional minute from emergency call to first shock was associated with:
- 6% lower survival to hospital discharge
- 6% higher probability of failed VF termination
- 4% lower probability of return to organized rhythm
Successful VF termination was 93% when delay was under 6 minutes and dropped to 75% when it exceeded 16 minutes. Dispatch delay is one of the most controllable variables in that timeline.
Cardiac arrest is the clearest example, but the exposure extends further. Delayed dispatch creates liability risk, erodes community trust, and can trigger regulatory scrutiny — particularly when delays trace back to coordination failures rather than travel time.
KPIs directly affected:
- Average dispatch time
- On-time arrival rate
- Response time compliance
- Emergency call-to-patient contact time
- Pickup delay rate
When this matters most: Peak call hours, mass casualty events, and agencies managing mixed ALS, BLS, and NEMT fleets simultaneously — where manual dispatch bottlenecks during high-volume periods.
Advantage 2: Optimized Resource and Crew Utilization
Scheduling software identifies the nearest unit and the correctly equipped one. Those aren't always the same vehicle.
In practice, the system factors in:
- Crew certifications — ALS vs. BLS qualification matching
- Vehicle configuration — wheelchair lifts, stretcher tie-downs, oxygen capacity
- Shift hours remaining — avoiding overtime and HOS violations
- Workload balance — distributing calls across the fleet rather than overloading available units
Without this logic, the default is "first available." That typically means dispatching an ALS unit to a routine NEMT transfer, or burning through one crew's shift while another sits idle. Both waste resources.
A 2019 tiered-dispatch study reviewing 1,220,820 EMS incidents found that for non-traumatic abdominal pain calls where the patient was alert and breathing, BLS ambulances alone handled 72.9% of cases with a mean response time of 8 minutes. Only 0.021% required emergent life-saving intervention. Protocol-driven triage backed by scheduling software enables that kind of appropriate unit matching at scale.
For EMS and NEMT operations building this into their dispatch stack, the underlying routing engine matters. NextBillion.ai's route optimization API supports 50+ hard and soft constraints — including skill-based crew matching, vehicle accessibility attributes, and shift-hour limits — with per-vehicle pricing that avoids the cost escalation typical of per-API-call billing at high dispatch volumes.
KPIs directly affected:
- Fleet utilization rate
- Crew overtime hours
- Idle time per vehicle
- Fuel consumption
- ALS/BLS unit balance
- Cost-per-transport
When this matters most: Operations managing 10+ vehicles, agencies mixing emergency and NEMT calls, and organizations facing crew shortages where optimal assignment — not just first available — is what sustains coverage.
Advantage 3: Compliance, Documentation, and Billing Accuracy
Every scheduling event — dispatch time, crew assigned, vehicle ID, patient handoff timestamp, transport completion — should generate an auditable record automatically. Purpose-built scheduling software does this at the point of service, not after the fact.
That documentation trail has direct financial consequences. CMS reported $595,144,661 in projected improper ambulance payments for the 2024 reporting period, at a 13.2% improper payment rate. The cause breakdown is telling: 63.5% of those improper payments were attributed to insufficient documentation. Not fraud. Not medical necessity disputes. Documentation gaps.
When scheduling and documentation are integrated, trip records flow directly into billing and compliance reporting. That eliminates the transcription errors that occur when crews reconstruct events from memory at the end of a back-to-back shift.
Accurate scheduling records also protect agencies during audits by providing a clear, timestamped timeline tied to specific crew credentials and vehicle certifications — the kind of detail CMS and state Medicaid auditors require for repetitive transport authorizations.
KPIs directly affected:
- Claim denial rate
- Documentation completion rate
- Billing cycle time
- Compliance audit outcomes
- Crew certification tracking accuracy
When this matters most: Agencies billing to Medicaid or Medicare, those undergoing state or federal audits, and operations where crews handle high volumes of back-to-back calls with limited time for manual documentation.
What Happens When Patient Transport Scheduling Is Manual or Fragmented
The operational consequences of phone-based dispatch, spreadsheets, or disconnected systems aren't hypothetical.
Virginia Beach EMS's CAD-down procedures show what manual fallback looks like in practice: unit availability tracked through a web-based matrix, with a magnetic board as the secondary option. Crews manually enter dispatch addresses and timestamps. Status changes go by radio. Any incidents captured on paper during the outage require re-entry after restoration.
For many EMS operations, this isn't an emergency workaround — it's the daily baseline.
Across operations that rely on manual coordination, the same failure patterns emerge:
- Dispatches the first available unit rather than the best-qualified one, wasting specialized resources
- Breaks down during peak hours, pushing time-sensitive cases past acceptable response windows
- Surfaces staffing gaps only after they appear, triggering last-minute overtime, burnout, and turnover
- Forces billing staff to manually reconcile trip logs, schedules, and patient records — extending claim timelines and multiplying error risk
- Hits a scaling ceiling defined by dispatcher cognitive capacity, not actual fleet availability
These issues don't stay separate. Delayed dispatch creates documentation gaps; documentation gaps cause billing denials; billing losses limit the budget for adding staff to address the coordination problem.
How to Get the Most Value from EMS Scheduling Software
Scheduling software delivers its full value when it's treated as an operational system, not a booking tool. That means integration, consistent use, and regular performance review.
Integration is where the gains compound fastest. Scheduling software connected to GPS/telematics, CAD systems, ePCR platforms, and billing tools eliminates data silos and ensures the scheduling layer reflects real-time ground truth. NextBillion.ai natively integrates with Samsara and Geotab: dispatchers can pull live vehicle data, optimize routes, and push assignments directly to driver apps without manual data handling.
Ride Care, a mental health transport operator, reduced route planning time from half a night to two hours after integrating NextBillion.ai's routing engine with their Samsara platform — and scaled from 60 to nearly 200 rides per day.
Ongoing performance review keeps the system working harder over time. Agencies that regularly analyze dispatch delay rates, utilization metrics, and documentation completion rates turn that data into concrete changes: updated routing logic, adjusted staffing patterns, and tighter compliance protocols. Without this review cadence, the software runs on day-one assumptions indefinitely.
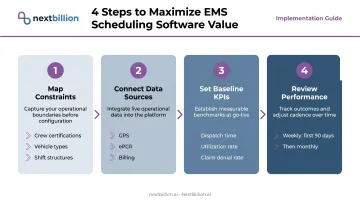
A few practical steps to maximize value:
- Map your current constraints before configuring the system: crew certifications, vehicle types, shift structures, and patient acuity categories all need to be represented in the scheduling logic
- Connect your data sources: GPS/telematics integration is the baseline, but ePCR and billing integration is what amplifies the compliance and documentation benefits
- Set baseline KPIs on day one — dispatch time, utilization rate, and claim denial rate are all measurable from the start
- Review performance weekly in the first 90 days, then monthly: the data only changes operations if someone is accountable for acting on it
Conclusion
Patient transport scheduling software's value runs through three areas: getting the right unit to the right patient faster, using crew and fleet resources more efficiently, and maintaining the documentation integrity that compliance and billing depend on.
These advantages don't operate in isolation. Better dispatch reduces clinical risk, which in turn makes resource allocation more defensible. Tighter resource matching lowers cost per transport. Cleaner documentation cuts claim denials. Each improvement compounds the others.
Agencies that integrate scheduling software with their existing systems, configure it accurately, and act on the data it surfaces can absorb rising call volumes without a proportional jump in coordination overhead. Sustainable EMS capacity isn't built by adding units alone. It's built by getting more out of the ones already in service.
Frequently Asked Questions
What is patient transport scheduling software for EMS?
Patient transport scheduling software automates vehicle, crew, and route assignments based on urgency level, crew certifications, and vehicle type. It uses real-time resource availability to replace manual phone or spreadsheet-based dispatch with rule-driven assignment logic.
How does scheduling software reduce response times in EMS?
By maintaining live visibility into unit location, crew availability, and vehicle configuration, the software makes dispatch decisions in seconds rather than minutes. That cuts the gap between call receipt and unit assignment, the most controllable segment of total response time.
Can EMS scheduling software integrate with existing CAD and dispatch systems?
Most modern platforms connect with CAD systems, GPS/telematics, and ePCR tools. API-first platforms enable deep integration without requiring a complete system replacement, allowing scheduling logic to sit on top of existing infrastructure.
What is the difference between EMS scheduling software and fleet management software?
Fleet management focuses on vehicle maintenance, location tracking, and fuel monitoring. Scheduling software handles assignment logic — matching the right crew and vehicle to each patient transport request in real time. Many modern platforms, including those that integrate with Geotab and Samsara, combine elements of both.
How does patient transport scheduling software help with regulatory compliance?
The software automatically logs dispatch events, crew assignments, and transport timelines, creating auditable records that simplify Medicaid, Medicare, and state compliance reporting. This directly addresses the documentation gaps that CMS identified as the leading cause of ambulance improper payments.
Is patient transport scheduling software suitable for both emergency and non-emergency medical transport?
Yes. Modern platforms handle both using urgency-based prioritization logic — emergency calls get immediate dispatch while NEMT and routine transfers are efficiently batched and routed without disrupting emergency coverage. ALS units, BLS units, and NEMT vehicles all operate within a single dispatch queue.