Introduction
A missed dialysis pickup isn't just an inconvenience. Miss it, and the patient may skip treatment entirely—with clinical consequences that can mean hospitalization within days. That's the operational reality facing NEMT dispatchers every morning.
According to MACPAC, over 3.2 million Medicaid beneficiaries used NEMT services in FY 2018, generating more than 60 million ride-days. With adults 65+ projected to reach 22% of the U.S. population by 2040, that volume is only growing.
The systems managing those rides haven't kept pace. Most NEMT operations still rely on phone-based scheduling, static spreadsheets, or routing software that locks in routes at shift start. Mid-day disruptions—a clinic running late, a driver calling out, an incomplete trip record—ripple into missed pickups and denied Medicaid claims.
What follows is a practical look at where traditional dispatch breaks down, what real-time and data-driven systems actually do differently, and what NEMT operators can expect when they close that gap.
Key Takeaways
- Manual dispatch creates cascading delays, double-bookings, and costly deadhead miles that compound across every shift
- Real-time dispatch continuously recalculates trip assignments using live GPS, traffic, and patient data throughout every shift
- NEMT routing requires 50+ constraints: vehicle type, driver certifications, time windows, patient acuity, and multi-stop sequencing
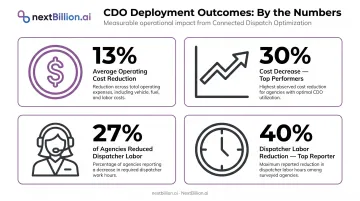
- CDO technology delivers an average 17% on-time performance improvement and 13% operating cost reduction, per ITS JPO research
- GPS-stamped trip logs are the foundation of Medicaid audit defense—manual driver logs don't hold up
Why Traditional Patient Transport Dispatch Falls Short
The Manual Scheduling Problem
Morning dialysis runs expose every weakness in manual dispatch. Coordinators are juggling phone confirmations, paper schedules, and shared spreadsheets while new trip requests come in. One driver running late ripples forward: the second pickup is now behind, the third gets rescheduled, and somewhere down the line a patient misses treatment.
Reactive scheduling can't absorb that kind of pressure. Double-bookings happen because two dispatchers don't see each other's assignments in real time. Missed pickups happen because there's no automated alert when a driver goes off-route. At scale, these failures are inevitable — they're built into how the system works.
Static Routes and Deadhead Miles
Routes built at 5 AM reflect conditions that won't exist by 8 AM. Traffic incidents, clinic delays, and patient cancellations all create gaps in a fixed schedule that dispatchers have to manually patch. The more trips a fleet runs, the wider those gaps become.
That gap has a direct cost: deadhead miles. Research from the Transportation Research Board found that dedicated demand-responsive paratransit operations can have deadhead miles accounting for as much as 50% of total revenue miles. Fuel, driver time, and vehicle wear — none of it producing a completed trip.
The Medicaid Documentation Exposure
Incomplete trip records aren't just an administrative nuisance—they're a financial liability. HHS-OIG audits have found the scale of this problem to be substantial:
- Massachusetts made at least $14.1 million in improper Medicaid NEMT payments due to inadequate documentation or non-qualifying services
- New York claimed $196 million—over 72% of the audited federal reimbursement amount—for NEMT payments that didn't meet Medicaid requirements
Manual driver logs can't produce the kind of verifiable, timestamped records that survive an audit. When Medicaid reviewers request proof of service, paper notes and spreadsheet entries rarely hold up.
What Real-Time Dispatch Actually Means in Patient Transport
Continuous Recalculation, Not Day-Start Planning
Real-time dispatch isn't just faster scheduling. It's a system that never stops recalculating. Live GPS positions, traffic feeds, driver availability, and patient eligibility status all feed into the engine continuously—not just at the beginning of a shift.
The National Academies define this as Continuous Dynamic Optimization (CDO): an automated process that evaluates new bookings, cancellations, and day-of-service events to re-optimize trip assignments without changing confirmed pickup windows.
When a patient cancels mid-morning, the system doesn't wait for a dispatcher to notice and manually reassign the gap. It recalculates immediately, compresses the route, and pushes an updated sequence to the driver's mobile app.
From Reactive to Predictive
Mature dispatch systems don't just respond to what's happening — they learn from what's happened before. Dialysis runs and oncology clusters repeat on predictable schedules; paratransit demand on specific corridors follows weekly rhythms. That trip history becomes a training dataset.
ML-driven routing learns from those patterns—flagging days when a specific clinic typically runs late, or when driver demand on a particular corridor spikes on Tuesday mornings. Fleet managers can pre-position vehicles and align schedules before peak periods arrive, rather than scrambling after they hit.
What Separates NEMT from General Logistics Dispatch
Generic routing tools are built for packages. Patient transport routing handles constraints that consumer mapping APIs don't model:
- Vehicle eligibility — wheelchair lift, stretcher, bariatric capacity
- Driver certifications — specialized training requirements for specific patient populations
- Patient acuity — distinguishing ambulatory riders from those needing assist
- Medicaid-approved pickup windows — time constraints tied to reimbursement, not just preference
- Multi-stop sequencing — home → clinic → pharmacy → home, with appointment windows at each leg
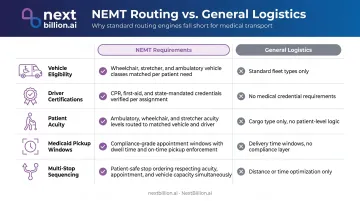
Miss any one of these constraints and the schedule looks valid on paper while failing in the field — a bariatric patient assigned a standard van, or a Medicaid pickup window missed by twelve minutes and flagged for recoupment.
The Data Feedback Loop
Every completed trip generates a record: actual vs. planned route, pickup deviation, wait time. Over time, these records refine future dispatch decisions. The system gets progressively more accurate as it accumulates trip history specific to each service area, driver, and appointment type.
ITS JPO data on CDO deployments shows what this produces in practice: agencies reported 8% to 31% increases in passenger trips per revenue vehicle hour, with an average on-time performance improvement of 17%.
Essential Capabilities for Data-Driven Patient Transport Logistics
Multi-Constraint Route Optimization
NEMT route optimization isn't a single variable problem. A compliant, efficient schedule must simultaneously satisfy:
- Vehicle type and accessibility configuration
- Driver qualifications and certifications
- Patient mobility requirements and acuity levels
- Hard and soft time windows for Medicaid-approved pickups
- Multi-stop sequencing with task dependencies
- Load capacity across multi-rider vehicles
NextBillion.ai's Route Optimization API supports more than 50 routing constraints covering all of these categories. That includes multi-dimensional capacity modeling for wheelchair vans and stretcher vehicles, skills-based driver matching, time window enforcement, and complex task sequences like pick-up → drop-off → wait → pick-up → drop-off.

The distance matrix scales to 5,000×5,000 elements—no 25×25 cap—making it viable for fleet-wide scheduling rather than individual trip planning.
Real-Time GPS Tracking and Driver Matching
Live GPS data serves two functions : it gives dispatchers accurate ETAs to share with patients, and it feeds the driver-vehicle matching engine.
NextBillion.ai's Driver Assignment API matches each incoming trip to the nearest qualified driver-vehicle combination. It checks location, shift timing, vehicle accessibility features, and driver certifications in under one second. For urgent same-day bookings, that response speed matters. Automated real-time reassignment handles mid-shift disruptions—driver call-outs, vehicle breakdowns—without manual dispatcher intervention.
Automated Compliance Documentation
CMS guidance requires trip records to include five specific fields:
- Beneficiary name and Medicaid ID
- Pickup and drop-off locations
- Service date and time
- Loaded miles
Manual driver logs produce all of these fields inconsistently.
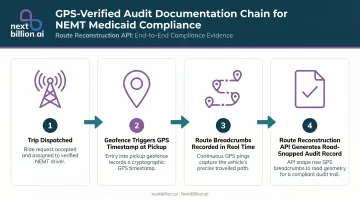
Geofence-triggered logging automatically timestamps each pickup and drop-off against GPS coordinates. NextBillion.ai's Route Reconstruction API transforms raw GPS breadcrumb sequences into road-snapped, audit-defensible trip records—every road taken, every waypoint, every distance mapped to the actual road network. HHS-OIG has specifically recommended GPS or electronic monitoring of NEMT drivers as an audit control, and these records are built to satisfy that standard.
System Integration and API Connectivity
A dispatch platform that operates in isolation creates a new data entry burden. The value comes from integration: trip data flowing automatically between the routing engine, telematics platforms, and billing systems.
NextBillion.ai offers native, bidirectional integrations with Samsara, Geotab, and Motive. Ride Care, a mental health and substance abuse transportation provider within Oklahoma's crisis response system, integrated NextBillion.ai's routing with their existing Samsara deployment.
Routes are optimized and pushed directly into drivers' Samsara apps—eliminating the manual data entry that previously introduced errors into every trip assignment.
Measurable Outcomes: What Operators Actually Gain
Cost Reduction and Dispatcher Productivity
The numbers from CDO deployments across ADA paratransit agencies are consistent:
- Average 13% operating cost reduction, with some agencies achieving up to 30% decreases (ITS JPO, 2023)
- 27% of surveyed agencies reduced dispatcher and scheduler labor costs; one reported a 40% reduction
- GOIN, a paratransit and NEMT provider handling 2,000 trips per day, achieved a 40% reduction in API costs and 30% reduction in driver idle time after switching to NextBillion.ai
For Ride Care, route planning that previously consumed half a night now takes under two hours. Dispatchers aren't eliminated—they're freed from mechanical trip assignment to focus on exception handling and patient communication.
Those dispatcher gains translate directly into on-time performance—and that's where the financial stakes get serious.
On-Time Performance and Patient Experience
On-time performance has direct financial implications under Medicaid contracts. The same ITS JPO research shows an average 17% improvement in on-time performance after CDO deployment.
Beyond contract compliance, accurate ETAs reduce patient anxiety, particularly for patients with chronic conditions who rely on predictable transport for weekly or daily appointments.
Research published in PMC found that among frequent healthcare users enrolled in Medicaid or Medicare, 35.3% delayed care and 18.3% missed appointments due to transportation problems. Real-time notifications and shorter wait times directly address both metrics.
For dialysis specifically, the stakes are highest: nearly 500,000 U.S. patients receive in-center hemodialysis, requiring more than 70 million roundtrips annually. Transportation issues are a leading cause of missed or shortened treatments—and missed treatments increase hospitalization risk.
Compliance and Medicaid Billing: Where Data Quality Is Non-Negotiable
Pre-Dispatch Eligibility Validation
Dispatching a ride to an ineligible beneficiary produces a non-reimbursable trip. North Carolina Medicaid requires eligibility verification for each month in which transportation is requested—a requirement that manual workflows routinely miss under volume pressure.
AI-enabled dispatch systems can query eligibility status before a trip is assigned. Non-qualifying trips never enter the schedule. This prevents both the direct cost of the unreimbursed ride and the downstream audit exposure when claim patterns trigger review.
GPS-Verified Trip Logs as Audit Infrastructure
The audit record must capture:
- Pickup and drop-off coordinates with GPS timestamps
- Actual route taken mapped to the road network
- Driver identity associated with each trip record
- Service duration from first door to last
NextBillion.ai's Route Reconstruction API generates road-snapped trip records from GPS breadcrumbs, creating documentation of what actually occurred rather than what was scheduled. These records are designed for regulated industries requiring verifiable trip history, including NEMT proof-of-service.
During a Medicaid audit, a GPS-reconstructed trip log is harder to challenge than a manual entry.
Automated Billing Code Generation
NEMT trips are billed using specific HCPCS codes. Applying the wrong code delays payment and triggers denial workflows. Common codes include:
- A0100 — Taxi or TNC transport
- A0130 — Wheelchair van
- A0080 — Volunteer vehicle mileage
Dispatch platforms that integrate with billing systems apply correct codes automatically based on vehicle type and trip attributes captured at the time of dispatch. Because the trip data already exists in the system, routing it directly to the billing workflow removes the manual re-entry step where most coding errors originate.
How NextBillion.ai Powers Patient Transport Dispatch Infrastructure
NextBillion.ai provides the routing and location intelligence infrastructure that NEMT software platforms and paratransit operators build on. The core capabilities purpose-built for patient transport include:
- 50+ routing constraints covering vehicle type, driver certifications, patient acuity, time windows, and multi-stop sequencing
- Distance matrix at 5,000×5,000 scale for fleet-wide ETA calculation without batching workarounds
- Sub-second Driver Assignment API matching the nearest qualified driver-vehicle combination to each trip request
- Native Samsara, Geotab, and Motive integrations with bidirectional data flow—no custom API development required
- Route Reconstruction API generating road-snapped, audit-defensible trip records for Medicaid proof-of-service
Ride Care's implementation shows what this looks like in production. Operating 24/7 psychiatric and substance use transportation across Oklahoma, Kansas, and Louisiana, they integrated NextBillion.ai with Samsara to handle constraints generic platforms couldn't model: ADA vehicle requirements, age separation rules for passengers, and driver HOS compliance.
Planning time dropped from half a night to under two hours. They now process 4,000–6,000 transports monthly and are expanding into new states.
Those operational gains only hold if the pricing model scales with them. NextBillion.ai's per-vehicle or per-order model contrasts directly with per-API-call pricing from generic mapping providers. As dispatch query volumes grow with fleet size, per-call costs spike unpredictably. GOIN's 2,000-trips-per-day operation generates roughly 800,000 distance matrix calls monthly — at per-call rates, costs spiral past any reasonable budget. With NextBillion.ai's volume-based pricing, GOIN reduced API costs by 40% while nearly doubling call volume.
NextBillion.ai's 2025 integration with Velocitor Solutions extends this further: NEMT operators can now access combined routing intelligence and fleet telematics in one platform, without stitching together separate vendor relationships.
Frequently Asked Questions
What is the dispatch software for medical transportation?
Medical transportation dispatch software automates trip assignment, route optimization, and compliance documentation for NEMT and paratransit providers. It replaces manual scheduling with AI-driven workflows that account for patient mobility needs, Medicaid eligibility, driver certifications, and time window requirements. General logistics software isn't built to model these constraints; purpose-built NEMT platforms are.
How does real-time dispatch reduce costs in patient transportation?
Real-time re-routing eliminates deadhead miles, reduces fuel consumption per shift, and allows smaller dispatcher teams to manage higher trip volumes. Industry research across paratransit agencies points to an average 13% operating cost reduction, with some operators reporting up to 30% decreases.
What routing constraints matter most for NEMT and paratransit fleets?
The critical constraints are vehicle type (wheelchair lift, stretcher, bariatric), driver certifications, patient acuity level, Medicaid-approved pickup time windows, and multi-stop trip sequencing. Generic routing APIs aren't built to hold all of these at once. Purpose-built NEMT routing engines, by contrast, support 50+ constraints across every category simultaneously.
How does data-driven routing improve Medicaid compliance in NEMT?
Automated GPS trip logs, pre-dispatch eligibility validation, and geofenced pickup confirmation create an audit-ready documentation trail. GPS-reconstructed records capture coordinates, timestamps, and route taken, producing records that hold up under Medicaid review and reducing claim denials tied to missing or incomplete documentation.
What is the difference between static and dynamic route optimization in medical transport?
Static routing is planned once at day start and can't adapt when circumstances change. Dynamic optimization continuously recalculates as cancellations, traffic incidents, and new requests occur throughout the shift. For NEMT fleets managing 50–200+ daily trips across variable appointment windows, static routing falls apart quickly — dynamic systems absorb those disruptions in real time.
How does GPS tracking and real-time dispatch improve patient experience?
Accurate ETAs and proactive notifications reduce patient anxiety, especially for those managing chronic conditions who rely on consistent transport for weekly treatments. Reliable arrival windows improve appointment adherence — a factor that affects both patient health outcomes and the provider's standing with Medicaid brokers.