Introduction
Automated patient transport scheduling is the technology-driven process of assigning vehicles, drivers, and routes to patient trips based on medical requirements, timing constraints, and fleet availability — with minimal manual intervention.
The stakes are different here than in standard logistics. When a freight shipment arrives late, someone reschedules. When a dialysis patient misses transport, they miss treatment. According to MACPAC, 5.2% of Medicaid beneficiaries — roughly 2.5 million people — delayed care because of transportation problems in 2018. That's not an inconvenience metric. It's a care access failure.
This guide covers how automated patient transport scheduling works operationally, what separates effective implementations from ineffective ones, and when the operational scale justifies the investment.
Key Takeaways
- Automated scheduling matches patients with vehicles using algorithm-driven logic across medical requirements, time windows, and driver qualifications — no phone coordination or spreadsheets
- Most critical in NEMT, hospital discharge transport, and paratransit — high trip volumes with strict payer compliance requirements
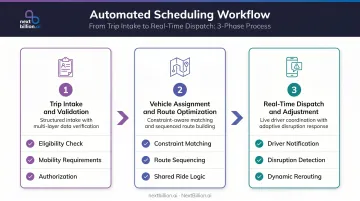
- Three core phases drive the process: trip intake and validation, vehicle assignment and route optimization, then real-time dispatch with dynamic adjustment
- Effectiveness depends on constraint complexity, data quality, EHR integration depth, and fleet size
- Small providers with low trip volumes may see better ROI from partial automation (documentation, billing) before moving to full dispatch automation
What Is Automated Patient Transport Scheduling?
Automated patient transport scheduling uses software to systematically intake trip requests, validate patient eligibility and medical requirements, and assign the most suitable vehicle and driver — all within rule-based or AI-assisted logic, replacing manual dispatcher decision-making.
The goal: every patient gets matched to the right vehicle type, at the right time, via the most efficient route — without schedulers juggling availability, vehicle specs, and patient needs across spreadsheets or phone calls.
What It Is Not
This distinction matters because the terms get conflated:
- GPS tracking monitors a trip already in progress — it operates downstream of scheduling
- Ride-hailing dispatch matches riders to generic vehicles without medical-grade constraints
- Automated scheduling operates upstream of both, handling trip creation, eligibility validation, and vehicle assignment before a driver ever gets a notification
A system that shows you where your vehicles are is a tracking system. One that decides which vehicle takes which patient, when, and why — that's automated scheduling.
Why Healthcare Logistics Depends on Automated Scheduling
The Scale Problem
Healthcare transport operations handle dozens to hundreds of trips per day across varying vehicle types, patient acuity levels, and appointment windows. CMS reported 81.3 million NEMT ride days in 2019, with 3 to 4 million Medicaid beneficiaries using NEMT annually. Among patients with end-stage renal disease, 47% used NEMT in 2021, averaging 5.5 monthly ride days each.
That's not occasional transport — it's recurring, high-frequency scheduling across a medically complex population. At that volume, manual coordination doesn't just become inefficient. It breaks.
According to TCRP research on computer-aided scheduling and dispatch, manual scheduling techniques typically become overwhelmed above roughly 1,000 trips per day.
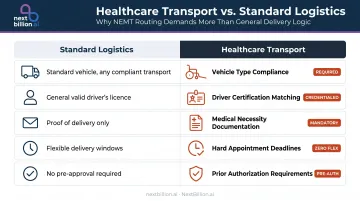
What Healthcare Demands That Standard Logistics Does Not
General freight can tolerate a late delivery. Patient transport cannot afford these failures:
- Vehicle type compliance — wheelchair, stretcher, or ambulatory vehicle must match patient need
- Driver certification matching — not every driver is qualified for every patient acuity level
- Medical necessity documentation — trips must be validated against payer eligibility before confirmation
- Hard appointment deadlines — a 9:00 AM dialysis appointment cannot be treated as approximate
- Prior authorization requirements — some payers require pre-authorization before a trip is rendered
The Compliance Dimension
For NEMT providers, compliance isn't a best practice — it's a billing prerequisite. CMS program integrity guidance identifies specific documentation elements providers must maintain: beneficiary name, Medicaid ID, pickup and drop-off locations, and date and time of service.
Billing for trips not rendered — including no-shows — is flagged as a fraud risk. GAO reported 189 NEMT criminal convictions or civil settlements from state Medicaid Fraud Control Unit investigations between 2015 and 2020. Automated scheduling creates auditable trip records that support payer reconciliation, accelerate audit responses, and reduce the conditions that enable both accidental errors and intentional fraud.
How Automated Patient Transport Scheduling Works
The process moves through three phases, with data flowing between patient records, scheduling logic, fleet systems, and driver-facing apps throughout.
Inputs the system works from:
- Trip requests (from healthcare staff, patients, care coordinators, or broker feeds)
- Patient medical profiles (mobility requirements, supervision needs, escort flags)
- Vehicle inventory data (type, current location, availability, accessibility features)
- Driver qualification records (certifications, shift status)
- Appointment time windows (hard deadlines vs. flexible arrival ranges)
Step 1: Trip Intake and Validation
The process begins when a trip request enters the system — via an online portal, EHR-integrated form, or broker feed. Before the trip enters the scheduling queue, the system validates:
- Medical necessity and payer eligibility
- Patient mobility requirements (ambulatory, wheelchair, stretcher)
- Requested time window against available capacity
- Prior authorization requirements, where applicable
Only validated trips proceed. This upstream check prevents downstream assignment errors and reduces the manual review burden on dispatchers.
Step 2: Vehicle Assignment and Route Optimization
Once validated, the scheduling engine matches each trip to available vehicles based on proximity, vehicle type, driver certification, and existing route load. This is where constraint-handling capacity becomes the critical differentiator.
Route optimization logic then sequences multiple trips per vehicle — including shared rides where medically appropriate — to minimize idle time, total mileage, and appointment latency while honoring hard constraints (wheelchair-accessible vehicle required, 9:00 AM hard arrival) and soft constraints (minimize detour time, prefer closer vehicle).
NextBillion.ai's Route Optimization API handles 50+ hard and soft constraints simultaneously in a single optimization run. For NEMT specifically, that includes:
- Multi-dimensional vehicle capacity — distinguishes between ambulatory, wheelchair, and stretcher vehicles
- Driver skill matching — enforces certification requirements per trip
- Time-window enforcement — honors hard appointment deadlines without compromise
max_time_in_vehiclethresholds — caps patient ride duration to clinical tolerances
Multi-stop shared rides — sequencing home → clinic → pharmacy → home across multiple patients on one vehicle — are a core supported use case.
Step 3: Real-Time Dispatch, Tracking, and Adjustment
Optimized routes push to drivers via mobile app. From there, the system monitors execution against planned schedules — and when disruptions occur (traffic delays, driver unavailability, patient no-shows, last-minute cancellations), dynamic rescheduling logic kicks in:
- Detects the change and removes or modifies the affected trip
- Recalculates impacted route sequences for other vehicles
- Notifies patients, facility staff, and dispatchers automatically
- Reassigns if necessary, within seconds
Ride Care, an NEMT operator working within Oklahoma's crisis response system, documented this shift directly: before automation, their team was "pasting trips together on sticky notes and working half the night." After deploying NextBillion.ai's route optimization, planning time dropped from most of a night to under two hours — while the operation scaled from 60 to nearly 200 rides per day.
Key Factors That Shape Scheduling Automation Effectiveness
Not every NEMT operation will see the same results from automation. Four factors determine how much value a provider actually captures.
Constraint Complexity
The more constraints a provider must honor per trip, the more the scheduling engine's constraint-handling capacity determines outcomes. A mixed fleet of ambulatory, wheelchair, and stretcher vehicles — each with different driver certification requirements and payer-specific documentation rules — needs a system that models all those combinations without forcing manual overrides.
One diagnostic question worth asking vendors directly: what happens when a trip has five simultaneous constraints? Does the system resolve it automatically, or does it escalate to a dispatcher?
Data Quality and Integration Depth
Automation is only as reliable as the data it runs on. Gaps in patient eligibility records, outdated vehicle availability feeds, or disconnected scheduling systems introduce errors that require human correction — partially defeating the efficiency gains.
Data integration choices also carry compliance implications. NextBillion.ai's platform optimizes using location coordinates rather than requiring PII in the routing layer — supporting HIPAA-compliant integration without exposing patient data in the optimization API itself.
Fleet Size and Trip Volume
Research from TCRP indicates manual scheduling becomes overwhelmed above approximately 1,000 trips per day. Below that threshold, the ROI calculation depends on operational specifics.
Small providers with predictable, low-volume schedules may not justify full dispatch automation — but partial automation (documentation generation, billing record creation, eligibility validation) often delivers measurable value at lower volume thresholds.
Real-world results back this up:
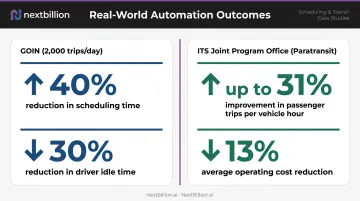
- GOIN (2,000 trips/day): 40% reduction in scheduling time, 30% reduction in driver idle time after deploying route optimization
- ITS Joint Program Office (paratransit): continuous dynamic optimization improved passenger trips per revenue vehicle hour by up to 31% and cut operating costs by 13% on average
Regulatory and Payer Environment
Medicaid, Medicare, and private insurers each impose different documentation, eligibility verification, and billing requirements. State NEMT programs vary further — Colorado's billing manual, for instance, requires actual pickup and drop-off times, driver name, vehicle identification, and trip logs for reimbursement.
Before selecting a platform, verify it can be configured for your specific payer rules and state documentation requirements — not just evaluated on generic routing benchmarks. A system that optimizes routes but can't produce Colorado-compliant trip logs creates compliance gaps that manual workarounds can't sustainably fix.
Common Misconceptions About Automated Patient Transport Scheduling
"Automation replaces dispatchers entirely."
It doesn't. Automated scheduling reduces dispatcher workload on routine assignments and documentation. Experienced dispatchers remain essential for exception handling, managing relationships with care teams, and scenarios the algorithm cannot resolve — a patient with unusual access requirements, a facility with undocumented loading restrictions, a same-day urgent trip with no obvious vehicle match.
"Route optimization alone equals automated scheduling."
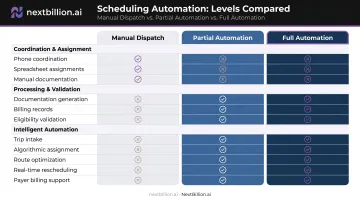
Route optimization is one component, not the whole system. Full automation also encompasses:
Route optimization is one component, not the whole system. Full automation also encompasses:
- Trip intake validation
- Driver-patient matching on non-route criteria (certification, vehicle type)
- Documentation generation
- Payer billing support
- Real-time rescheduling
A fleet that optimizes routes but handles these steps manually is only partially automated.
"Any scheduling software qualifies as 'automated'."
True automation uses algorithmic or AI-driven logic to make assignment decisions. Software that digitizes manual processes — electronic calendars, basic booking forms — is a different category entirely. Providers using those tools may still be doing most scheduling work by hand, just with a digital interface instead of paper.
The diagnostic question: does the system make assignment decisions, or does it record the decisions a human already made?
Frequently Asked Questions
What is the difference between automated patient transport scheduling and manual NEMT dispatch?
Manual dispatch relies on a human coordinator reviewing trip requests and making vehicle assignments by phone or spreadsheet. Automated scheduling uses algorithm-driven logic to match trips to vehicles, optimize routes, and push assignments to drivers with minimal human intervention — reducing both processing time and assignment errors.
How does automated scheduling handle last-minute trip changes or cancellations?
Most automated systems include dynamic rescheduling logic that detects a cancellation or change, removes or modifies the affected trip, recalculates impacted route sequences, and notifies drivers and facility contacts in real time — typically faster than a dispatcher could manually coordinate the same change.
What compliance requirements should automated patient transport scheduling systems address?
Systems should support HIPAA data privacy, Medicaid/Medicare trip documentation standards (beneficiary identity, pickup/drop-off times, vehicle and driver records), state-level NEMT eligibility verification, and automatic generation of trip-level audit records — produced as part of standard trip processing for providers billing government payers.
Can automated patient transport scheduling integrate with existing hospital EHR systems?
Most enterprise-grade scheduling platforms offer API-based EHR integration. For Epic or Oracle Health specifically, providers should validate the exact transport-request capabilities with the vendor before assuming full EHR initiation support — native compatibility varies significantly.
At what scale does automated patient transport scheduling become cost-effective?
TCRP research suggests manual scheduling becomes overwhelmed above roughly 1,000 trips per day. Below that threshold, ROI depends on payer complexity, vehicle mix, and recurring trip density. Documentation and billing automation typically deliver measurable value first — making them a practical entry point for smaller operations before full dispatch automation is warranted.
What cost reductions are associated with automated patient transport scheduling?
Current research doesn't support a universal savings figure for NEMT automation. The ITS Joint Program Office documented a 13% average operating cost reduction and 56% average customer complaint reduction in paratransit operations using continuous dynamic optimization — the most concrete benchmarks available.